RT4 Xenograft Model Overview
The RT4 xenograft model is derived from a human grade I papillary urothelial carcinoma of the bladder and is widely regarded as a reference system for studying well-differentiated, luminal-type non–muscle-invasive bladder cancer (NMIBC). The RT4 cell line was established from a primary bladder tumor and retains robust epithelial differentiation, minimal invasiveness, and a highly organized growth architecture both in vitro and in vivo. As such, it serves as a biologically stable and clinically relevant model for evaluating therapies aimed at early-stage bladder cancer and for elucidating the molecular underpinnings of urothelial differentiation.
Unlike high-grade invasive models such as T24 or UM-UC-3, RT4 represents a non-aggressive, low-grade tumor phenotype, with limited proliferation, intact DNA damage response, and preserved cell–cell adhesion. It is most suitable for mechanistic studies of differentiation therapy, retinoid signaling, chromatin remodeling, and receptor modulation in well-differentiated tumors. Because of its slower growth kinetics and histological fidelity to early-stage disease, RT4 is frequently used in proof-of-concept drug validation, long-term dosing studies, and pharmacodynamic profiling of urothelial maintenance strategies.
Request a Custom Quote for RT4 Xenograft ModelBiological and Molecular Characteristics
RT4 cells exhibit strong epithelial morphology and retain markers associated with terminal urothelial differentiation, including uroplakin II, cytokeratin 20, and GATA3. The cell line is wild-type for TP53 and RB1, and maintains normal apoptotic and cell cycle checkpoint responses. Unlike basal or squamous subtypes, RT4 expresses high levels of E-cadherin, CK18, and FOXA1, with no evidence of EMT or dedifferentiation under standard culture conditions.
Signaling pathway activity is tightly regulated, with low basal activation of PI3K/AKT, ERK1/2, and EGFR pathways. FGFR3 is moderately expressed but not mutated, and the cell line lacks the oncogenic amplifications that drive aggressive behavior in more advanced models. Chromosomal stability is comparatively high, and the overall mutation burden is low, consistent with its indolent phenotype.
| Characteristic | RT4 Profile |
|---|---|
| Origin | Human bladder, grade I papillary urothelial carcinoma |
| TP53 Status | Wild-type |
| RB1 Status | Wild-type |
| Differentiation Markers | Uroplakin II+, CK20+, GATA3+, FOXA1+ |
| Epithelial Markers | E-cadherin+, CK18+, CK7+ |
| Basal/Squamous Markers | Absent (CK5-, CK14-, ΔNp63-) |
| FGFR3 Status | Wild-type (moderate expression) |
| EGFR/PI3K/ERK Activity | Low basal |
| EMT Profile | Absent |
| Apoptotic Function | Intact (caspase-responsive) |
These features make RT4 ideal for modeling non-invasive bladder tumor biology, epithelial stability, and targeted therapies that rely on intact tumor suppressor pathways.
In Vivo Model Development and Tumorigenicity
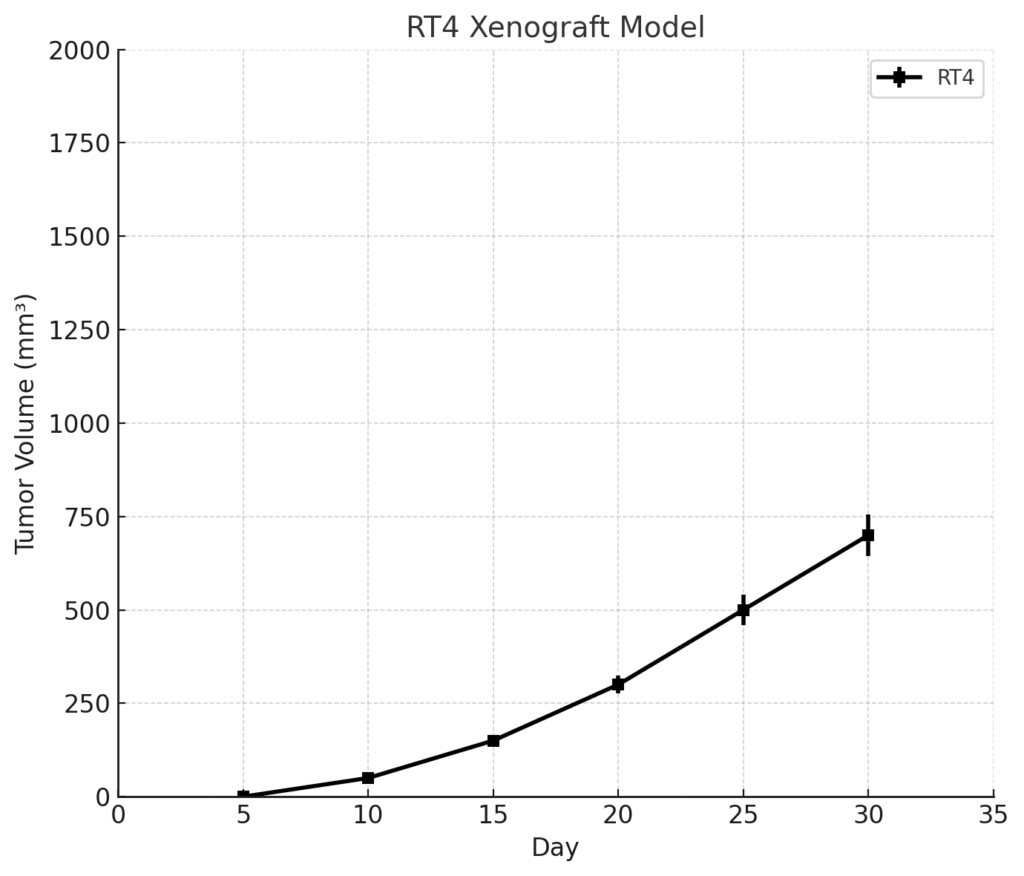
RT4 xenografts form slowly growing, well-differentiated tumors in immunodeficient mice, with take rates around 70–80% depending on implantation conditions. Subcutaneous inoculation of 1 × 10^7 cells in Matrigel produces measurable tumors within 2–3 weeks, with endpoint volumes (~1,000–1,200 mm³) typically reached over 5–6 weeks. Due to its low proliferative index, RT4 is particularly well suited for long-term studies, maintenance therapy evaluations, and investigations into tumor dormancy.
Orthotopic implantation models using bladder wall injection or intravesical instillation have been explored to recapitulate localized, non-invasive disease. These models preserve the non-metastatic, well-differentiated nature of RT4 tumors, and are compatible with luminal marker tracking and urothelial barrier studies. In vivo growth is compact, avascular, and non-invasive, enabling high-fidelity modeling of early-stage bladder cancer.
RT4 xenografts are amenable to immunohistological, pharmacodynamic, and differentiation state assessments. Bioluminescent tagging can be used for long-term imaging studies, although the slow progression of tumors necessitates extended observation periods.
Request a Custom Quote for RT4 Xenograft ModelHistopathology and Immunohistochemical Profile
Histologically, RT4 xenograft tumors display classical papillary architecture with fibrovascular cores, cohesive epithelial nests, and minimal nuclear pleomorphism. Tumor cells are columnar to cuboidal with abundant cytoplasm, small round nuclei, and infrequent mitoses. Necrosis and stromal invasion are virtually absent, consistent with the indolent clinical behavior of the original tumor.
Immunohistochemical staining reveals strong membranous E-cadherin expression and nuclear GATA3 positivity, confirming luminal subtype identity. CK20 and uroplakin II are expressed throughout the tumor epithelium, while Ki-67 proliferation index remains low (15–25%). RT4 tumors show minimal EGFR expression and little to no activation of phospho-AKT or phospho-ERK1/2, in contrast to more aggressive models.
Markers of EMT such as vimentin and N-cadherin are undetectable, and CD31 staining indicates sparse vasculature. This phenotypic stability and preserved epithelial character make RT4 histology a gold standard for modeling non-invasive urothelial differentiation in vivo.
Preclinical Applications and Drug Response
The RT4 xenograft model is widely used for investigating agents that promote differentiation, suppress urothelial proliferation, or maintain epithelial architecture. Due to its intact TP53 and RB1 function, RT4 is responsive to DNA-damaging agents, including mitomycin C and epirubicin, which are standard intravesical therapies in NMIBC. It also demonstrates sensitivity to retinoids, HDAC inhibitors, and histone methyltransferase inhibitors, all of which promote terminal differentiation or chromatin remodeling.
Because of its epithelial integrity and low invasiveness, RT4 is not appropriate for modeling metastatic disease or chemoresistant behavior. However, it is optimal for longitudinal therapeutic studies, pharmacodynamic monitoring, and combination regimens that aim to restore tumor suppressive control or prevent progression to invasive phenotypes.
Recent applications include testing of FGFR inhibitors, urothelial barrier modulators, and bladder-selective cytotoxic agents, especially in orthotopic models mimicking NMIBC. RT4 is also useful for assessing drug retention, mucosal penetration, and treatment scheduling relevant to intravesical drug delivery strategies.
Request This Model
To request the RT4 xenograft model or incorporate it into differentiation therapy screens, intravesical drug studies, or early-stage bladder cancer modeling, please use the form below. Our team will assist with study design, scheduling, and integration into your research workflow.
Request a Custom Quote for RT4 Xenograft Model